


Heal:
Anxiety - High Cholesterol - The Gut - The Heart - The Liver - Inflammation - The Kidneys - The Lymphatic System - The Nervous System - The Pancreas - The Pineal Gland - The Reproductive System - The Thyroid
Anxiety - High Cholesterol - The Gut - The Heart - The Liver - Inflammation - The Kidneys - The Lymphatic System - The Nervous System - The Pancreas - The Pineal Gland - The Reproductive System - The Thyroid
Heal Your Heart
When I looked at the heart for the first time I saw a circumferential basal loop. And then I saw a descending limb and an ascending limb. And they curl around each other at a helix and a vortex, except for the ventricle. And the angles at which they go is about 60 degrees. 60 degrees down and 60 degrees going up, and they cross each other in that way. For years people had wondered why this happened. I realized this is really a spiral. And I began to think about spirals. And I began to understand that spirals are almost the master plan of nature in terms of structure and in terms of rhythm… if you pick the middle of the spiral up you form a helix. And of course the heart is a helix.
Gerald Buckberg, MD
Gerald Buckberg, MD
With regard to the influences on the heart, we certainly have a relationship to the movements of cosmic bodies, especially the moon. If you make your heart such that you look at your blood circulation through your body, as it were, and do not have inner sensation of the heart, nor of your pulse beat, but through them, if you learn to through yourselves – you will see not just the blood circulation but you’ll see the whole movement of the moon, everything the moon does, and you’ll see how the moon relates to the sun. And you will then see the relationship which the heart has to sun and moon.
Rudolf Steiner
Rudolf Steiner
The heart is the household divinity which, discharging its function, nourishes, cherishes, quickens the whole body, and is indeed the foundation of life, the source of all action.
William Harvey
William Harvey
The ancient medicine of great cultures found in China and India, Egypt and extending throughout the world have described the heart in a more esoteric sense while simultaneously alluding to and offering valuable clues as to the true nature of the heart: It's form and function being interwoven, the mystery of the heart is revealed: the once thought mass of flesh being unwound into its true spiral form, the sacred helix. It is our privilege to connect the modern dots, as it were, to the ancient knowledge and likewise in a sense our responsibility to shift the paradigm of the heart as it is currently seen, from a mechanical pump, to a more elegant concept of sacred geometries, a model of pure brilliance created in the image of the Universe itself.
This is the New Earth Science, the merge of science and sacred, or more accurately said, the recognition of science as sacred.
This is the New Earth Science, the merge of science and sacred, or more accurately said, the recognition of science as sacred.
Heart Discovery Timeline
10,000-8,000 B.C.E.
The heart symbol, the popular icon for the heart, can be traced to before the last Ice Age, where Cro-Magnon hunters in Europe used the symbol in pictograms.
2,500-1,000 B.C.E.
The Egyptians believe the heart, or the ieb, is the center of life and morality. Egyptian mythology states that after death, your heart is taken to the Hall of Maat, the goddess of justice. There your heart is weighed against the Feather of Maat.
400-200 B.C.E.
Ancient Greeks hold the heart to be the center of the soul and the source of heat within the body. Scholars and physicians such as Hippocrates and Aristotle see the connection between the heart and lungs and seem to be aware of its action.
130-200
Galen makes several important observations concerning the heart, including the description of valves and ventricles and the differences between veins and arteries.
1000-1400
During the Middle Ages, the methods of Galen and other ancient physicians are strictly followed, and there are no new medical advances concerning the heart.
1500-1600
Scholars begin to question accepted views of the heart. Scholars and physicians such as Andreas Vesalius, the father of modern anatomy, and Michael Servitus make several key observations about the anatomy of the heart, while Leonardo da Vinci produces his sketch of the organ.
1628 - William Harvey publishes "An Anatomical Study of the Motion of the Heart and of the Blood in Animals," which details for the first time the idea of circulation and how blood travels throughout the body, propelled by the heart.
1908 - James B. Pettigrew, Professor of Medicine at St. Andrews University (Scotland), performed dissections of the heart and discovered that the heart muscle has seven muscle layers. Pettigrew postulated that one group of muscles contracts during systole while the other stores energy that is utilized in diastole. In his view, the motion of the heart muscle is like that of a torsional (twisting) pendulum.
1920 - Rudolf Steiner asserts in various lectures to medical doctors that the heart is not a pump forcing inert blood to move with pressure but that the blood is propelled with its own biological momentum, as can be seen in the embryo, and boosts itself with "induced" momenta from the heart. He also stated that the pressure does not cause the blood to circulate but is caused by interrupting the circulation. (2)
1932 - Harvard University scientist J. Bremer filmed the blood flow in embryos before the formation of the heart valves. He observed that the spiraling blood is boosted by the pulsating heart without creating turbulence in the blood. He described two streams in the heart tubes that spiral with different forward velocities around their own longitudinal axes and around each other (Presence and influence of spiral streams in the heart of the chick embryo, American Journal of Anatomy, 49: 409-440). Bremer’s findings were confirmed in 1981 by the surgical studies of A. Arbulu and I. Asfaw: “Not only is the blood flow well maintained in the embryo before the formation of the valves; there are reports of adults in whom both infected tricuspid and pulmonary valves were surgically removed and not replaced by prosthetic valves, without significant problems”.
1973 - Francisco Torrent-Guasp describes the structure of the heart as a band of muscle that starts at the pulmonary artery entry-point and ends below the aorta exit, wrapping itself into a double helical coil that bounds both ventricular cavities with a wall to separate them. Taking this architecture as his basis, in 1997 he presented a theory that provided an explanation as to how progressive contraction of the band accounted for the ejection and suction of the blood.
1995 - Ralph Marinelli of Temple University in Philadelphia refutes the pump propulsion theory: “When the heart begins to function, it enhances the blood's momentum with spiraling impulses. The arteries serve a subsidiary mimical heart function by providing spiraling boosts to the circulating blood. In so doing the arteries dilate to receive the incoming blood and contract to deliver an impulse to increase the blood's momentum.” (The Heart is not a Pump, 1995)
The heart symbol, the popular icon for the heart, can be traced to before the last Ice Age, where Cro-Magnon hunters in Europe used the symbol in pictograms.
2,500-1,000 B.C.E.
The Egyptians believe the heart, or the ieb, is the center of life and morality. Egyptian mythology states that after death, your heart is taken to the Hall of Maat, the goddess of justice. There your heart is weighed against the Feather of Maat.
400-200 B.C.E.
Ancient Greeks hold the heart to be the center of the soul and the source of heat within the body. Scholars and physicians such as Hippocrates and Aristotle see the connection between the heart and lungs and seem to be aware of its action.
130-200
Galen makes several important observations concerning the heart, including the description of valves and ventricles and the differences between veins and arteries.
1000-1400
During the Middle Ages, the methods of Galen and other ancient physicians are strictly followed, and there are no new medical advances concerning the heart.
1500-1600
Scholars begin to question accepted views of the heart. Scholars and physicians such as Andreas Vesalius, the father of modern anatomy, and Michael Servitus make several key observations about the anatomy of the heart, while Leonardo da Vinci produces his sketch of the organ.
1628 - William Harvey publishes "An Anatomical Study of the Motion of the Heart and of the Blood in Animals," which details for the first time the idea of circulation and how blood travels throughout the body, propelled by the heart.
1908 - James B. Pettigrew, Professor of Medicine at St. Andrews University (Scotland), performed dissections of the heart and discovered that the heart muscle has seven muscle layers. Pettigrew postulated that one group of muscles contracts during systole while the other stores energy that is utilized in diastole. In his view, the motion of the heart muscle is like that of a torsional (twisting) pendulum.
1920 - Rudolf Steiner asserts in various lectures to medical doctors that the heart is not a pump forcing inert blood to move with pressure but that the blood is propelled with its own biological momentum, as can be seen in the embryo, and boosts itself with "induced" momenta from the heart. He also stated that the pressure does not cause the blood to circulate but is caused by interrupting the circulation. (2)
1932 - Harvard University scientist J. Bremer filmed the blood flow in embryos before the formation of the heart valves. He observed that the spiraling blood is boosted by the pulsating heart without creating turbulence in the blood. He described two streams in the heart tubes that spiral with different forward velocities around their own longitudinal axes and around each other (Presence and influence of spiral streams in the heart of the chick embryo, American Journal of Anatomy, 49: 409-440). Bremer’s findings were confirmed in 1981 by the surgical studies of A. Arbulu and I. Asfaw: “Not only is the blood flow well maintained in the embryo before the formation of the valves; there are reports of adults in whom both infected tricuspid and pulmonary valves were surgically removed and not replaced by prosthetic valves, without significant problems”.
1973 - Francisco Torrent-Guasp describes the structure of the heart as a band of muscle that starts at the pulmonary artery entry-point and ends below the aorta exit, wrapping itself into a double helical coil that bounds both ventricular cavities with a wall to separate them. Taking this architecture as his basis, in 1997 he presented a theory that provided an explanation as to how progressive contraction of the band accounted for the ejection and suction of the blood.
1995 - Ralph Marinelli of Temple University in Philadelphia refutes the pump propulsion theory: “When the heart begins to function, it enhances the blood's momentum with spiraling impulses. The arteries serve a subsidiary mimical heart function by providing spiraling boosts to the circulating blood. In so doing the arteries dilate to receive the incoming blood and contract to deliver an impulse to increase the blood's momentum.” (The Heart is not a Pump, 1995)
Heart Explorers
James Pettigrew
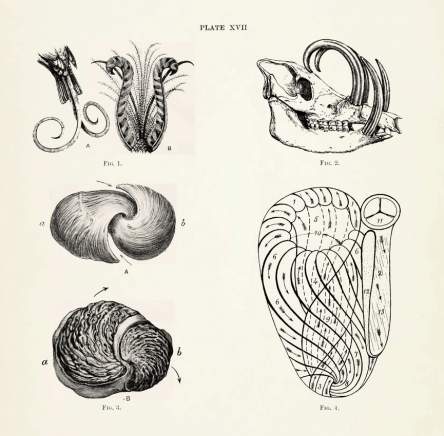 Plate XVII from the first volume of Pettigrew’s Design in Nature (1908), illustrating 'spiral formations in feathers and teeth, in the muscular arrangements of the heart, and in the cast of the ventricular cavities of the heart.'
Plate XVII from the first volume of Pettigrew’s Design in Nature (1908), illustrating 'spiral formations in feathers and teeth, in the muscular arrangements of the heart, and in the cast of the ventricular cavities of the heart.'
James Bell Pettigrew (1834 – 1908) was a Scottish anatomist and noted naturalist. As a medical student at the University of Edinburgh he developed a programme of research into the morphology of the human heart. During this project he prepared 112 dissections of cardiac muscle recording these by meticulous drawings and photographs. For this work he was awarded the anatomy gold medal. Pettigrew was invited to deliver the Croonian Lectures of the Royal Society and the Royal College of Physicians of London in 1860. In these lectures Pettigrew advanced a remarkable discussion of the anatomical arrangement of the musculature of the heart.
Pettigrew delivered his address, “On the Arrangement of the Muscular Fibres in the Ventricles of the Vertebrate Heart”, to the Royal Society the very same week that Origin of Species was published by John Murray of Albemarle Street, a short walk from the Royal Society lecture hall. That anyone might attribute such an ingeniously crafted organ as the mammalian heart to mere chance, Pettigrew believed, was sheer madness.
Nature’s variegated spiral structures, with the mammalian heart always for him the epitome, represented but one panel of the triptych that Pettigrew would go on to assemble over the next half century. Volume Two of Design in Nature is devoted solely to spiral movement in circulation (although the circulation section dealt with both plant and lower animal circulatory systems, three-quarters of this study focused on mammals and man); Volume Three to the spiral as locomotion’s characteristic form. In both arenas of animal physiology, Pettigrew found a spectacular resonance: movement at once precedes and follows structure, the direction of movement in living things being in every instance determined by the composition and configuration of kinetic spiral parts. This resonance seemed to reach right down to the atomic level. Unlike the closed system of the heart, the spiraling lines of atoms and molecules were arranged so that matter could be added in any amount, in unlimited directions. An open flow of energy and form was the basis for growth and progression in all creatures.
Pettigrew delivered his address, “On the Arrangement of the Muscular Fibres in the Ventricles of the Vertebrate Heart”, to the Royal Society the very same week that Origin of Species was published by John Murray of Albemarle Street, a short walk from the Royal Society lecture hall. That anyone might attribute such an ingeniously crafted organ as the mammalian heart to mere chance, Pettigrew believed, was sheer madness.
Nature’s variegated spiral structures, with the mammalian heart always for him the epitome, represented but one panel of the triptych that Pettigrew would go on to assemble over the next half century. Volume Two of Design in Nature is devoted solely to spiral movement in circulation (although the circulation section dealt with both plant and lower animal circulatory systems, three-quarters of this study focused on mammals and man); Volume Three to the spiral as locomotion’s characteristic form. In both arenas of animal physiology, Pettigrew found a spectacular resonance: movement at once precedes and follows structure, the direction of movement in living things being in every instance determined by the composition and configuration of kinetic spiral parts. This resonance seemed to reach right down to the atomic level. Unlike the closed system of the heart, the spiraling lines of atoms and molecules were arranged so that matter could be added in any amount, in unlimited directions. An open flow of energy and form was the basis for growth and progression in all creatures.
Design In Nature: Illustrated By Spiral And Other Arrangements In The Inorganic And Organic Kingdoms As Exemplified In Matter, Force, Life, Growth... In Crystals, Plants, And Animals (Volumes 1-3)
Francisco Torrent-Guasp
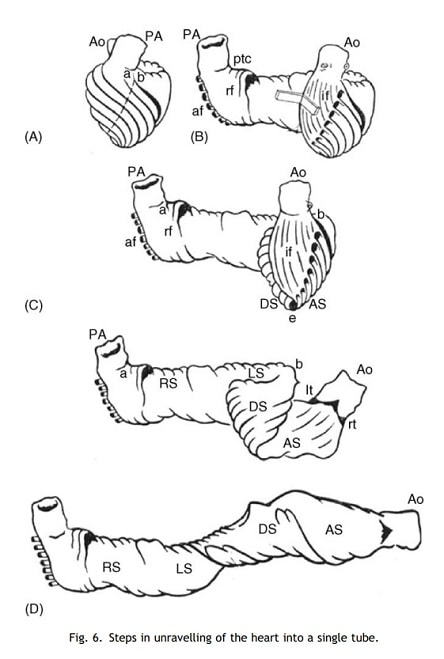
Paco Torrent-Guasp was born in Gandía (1931), in the duchy of the Borggia, the driving force behind the culture of the Quattrocento, but he lived and researched in Denia, a Roman, Moorish and always Mediterranean city. He read Medicine in Madrid and Salamanca and soon, in 1954 while still a student, he became interested in the heart’s functioning. He never believed that blood could enter the left ventricle without the help of suction. Paco thought it strange that from Harvey’s historic denial to Erasistratus and Galen an impossible mechanism should be considered viable. In fact, whenever he named the vis a tergo* he would laugh and wink, conspiratorially enjoining you to disbelief, too. He began with microscope studies that gave him no answers and followed by dissecting hearts from all kinds of animals. In 1973, for the first time in history, he described the structure of the heart as a band of muscle that starts at the pulmonary artery entry-point and ends below the aorta exit, wrapping itself into a double helical coil that bounds both ventricular cavities with a wall to separate them (Figure 6). Taking this architecture as his basis, in 1997 he presented a theory that provided an explanation as to how progressive contraction of the band accounted for the ejection and suction of the blood. By then, it was 43 years later.
(Juan Cosín Aguilar Centro de Investigación La Fe, Valencia, Spain.) (4)
*vis-a-tergo translated from Latin ‘A force acting from behind; a propulsive force;' Cardiology term referring to the force driving the venous return of peripheral blood, which is supplied by the left ventricle; by the time blood has passed through the capillaries, the blood pressure, or vis-a-tergo, is 15 mm Hg
I was privileged to observe him while he carefully blunt-dissected the heart. His plan, as he explained to me, was to dissect from apex to base, starting at the apex. Finally, the whole heart was gradually dissected with his bare fingers, after heating the organ to loosen its collagen fibres. The increasingly fascinating layers of tissue he produced revealed muscle fibres apparently disappearing into the apex of the heart and these fibres were clearly demonstrated for the first time. This point I would designate respectfully as ‘Guasp’s Point’. Already a ‘figure-of[1]eight’ type of muscle pattern was appearing, although at that time we had no understanding of its significance. In 1973 he published his preliminary findings (Fig. 3). Torrent-Guasp was a prolific and descriptive writer, and particularly excellent at illustrations, which helped his otherwise technical and linguistic difficulties in making himself understood. A clear figure-of-eight type of muscle pattern emerged, beautifully and sometimes frighteningly illustrated (Fig. 4), with the fibres disappearing at the cardiac apex, and this was in direct contrast to what, at that time, was accepted dogma; namely, that the myocardial muscle fibres ran from the mitral valve ring directly to the apex.
Finally, with regard to the suggested eponym ‘The Torrent-Guasp Heart’, incorporating both form and function: I regard this title as wholly appropriate, and probably more suitable than the more cumbersome and perhaps ill-under[1]stood ‘Helical Ventricular Myocardial Band’. Unless there is a more appropriate suggestion to clarify Paco’s legacy, I propose we should accept this term ‘The Torrent-Guasp Heart’ to establish and perpetuate his unique contributions. (Editorial by Donald Ross titled Torrent-Guasp’s Anatomical Legacy published 2006)
(Juan Cosín Aguilar Centro de Investigación La Fe, Valencia, Spain.) (4)
*vis-a-tergo translated from Latin ‘A force acting from behind; a propulsive force;' Cardiology term referring to the force driving the venous return of peripheral blood, which is supplied by the left ventricle; by the time blood has passed through the capillaries, the blood pressure, or vis-a-tergo, is 15 mm Hg
I was privileged to observe him while he carefully blunt-dissected the heart. His plan, as he explained to me, was to dissect from apex to base, starting at the apex. Finally, the whole heart was gradually dissected with his bare fingers, after heating the organ to loosen its collagen fibres. The increasingly fascinating layers of tissue he produced revealed muscle fibres apparently disappearing into the apex of the heart and these fibres were clearly demonstrated for the first time. This point I would designate respectfully as ‘Guasp’s Point’. Already a ‘figure-of[1]eight’ type of muscle pattern was appearing, although at that time we had no understanding of its significance. In 1973 he published his preliminary findings (Fig. 3). Torrent-Guasp was a prolific and descriptive writer, and particularly excellent at illustrations, which helped his otherwise technical and linguistic difficulties in making himself understood. A clear figure-of-eight type of muscle pattern emerged, beautifully and sometimes frighteningly illustrated (Fig. 4), with the fibres disappearing at the cardiac apex, and this was in direct contrast to what, at that time, was accepted dogma; namely, that the myocardial muscle fibres ran from the mitral valve ring directly to the apex.
Finally, with regard to the suggested eponym ‘The Torrent-Guasp Heart’, incorporating both form and function: I regard this title as wholly appropriate, and probably more suitable than the more cumbersome and perhaps ill-under[1]stood ‘Helical Ventricular Myocardial Band’. Unless there is a more appropriate suggestion to clarify Paco’s legacy, I propose we should accept this term ‘The Torrent-Guasp Heart’ to establish and perpetuate his unique contributions. (Editorial by Donald Ross titled Torrent-Guasp’s Anatomical Legacy published 2006)
Frank Chester
 Frank Chester’s chestahedron is a seven-sided form made of four equilateral triangles and three kite-shaped quadrilaterals.
Frank Chester’s chestahedron is a seven-sided form made of four equilateral triangles and three kite-shaped quadrilaterals.
Through his knowledge of anthroposophy, Chester knew that, according to some people, Steiner had described the heart as a seven-sided form that sits in an imaginary box in the chest. Chester became intrigued with this idea and wondered if anyone had ever tried to model such a thing. He set out to sculpt this form. After many failed attempts, Frank succeeded in sculpting a chestahedron: a seven-sided form of four equilateral triangles and three kite—shaped quadrilaterals with equivalent surface areas, twelve edges, and three different symmetries. This seemingly humble achievement offers some dramatic insights into the form and function of the human heart. Frank’s next step, as Steiner might have suggested, was to put this seven—sided form into a box—that is, the tightest cube it could fit into. In other words, imagine taking this form, facing the point down and just fitting it into a “regular” box. The apex, or point, does not fall in the center of the cube, but rather slightly off—center. Specifically, the chestahedron sits at an angle of 36 degrees off of center. Amazingly, this is the same angle at which the heart sits within the chest:
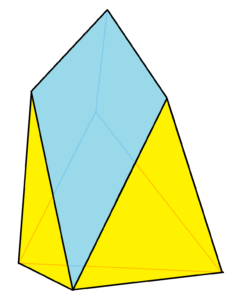
The Chestahedron is a geometric polyhedron. It is a 3-fold rotational prismatic symmetrical heptahedron.
It is the first known seven-sided solid with faces of equal area. (1)
Thomas Cowan
Tom Cowan is an Anthroposophical Medical Doctor, also inspired by Rudolf Steiner's insights on the heart. Cowan writes a text interweaving his personal experience as a medical student and doctor, the questions and missing spaces of how the heart and circulation is currently taught, providing valuable insight as to how Steiner's Heart fills in those missing spaces. Of particular interest is Cowan's accurate and insightful description of how the blood moves through the heart, using examples of how the hydraulic ram, as described by Steiner may be used as a model for certain actions in the heart producing different flows of laminar and vortex patterns and how this phenomena gives a coherent explanation for how the heart vortexes the blood through it, (without the existence of or need for a powered pump or pressure propulsion) boosting its momenta as it is released into the aorta.
If you examine the relative velocity of the blood at various stages of the circulation, you’ll see that the blood moves the fastest in the large arteries and veins, where it is forced into comparatively fewer channels, and the blood moves the slowest in the capillaries, because there are so many of them. This is similar to how water moves in a river. It is fastest when the river is narrow, slower when it flows out into tributaries, and slowest when it flows out into a wetland area.
What’s amazing is that blood actually stops moving in the capillaries, which is necessary for the efficient exchange of gases, nutrients, and waste products. After the blood stops moving, it oscillates slightly, and then begins to flow again as it enters the veins. But if the blood stops moving at the midpoint of its circular flow through blood vessels, only then to start moving again, what is the force that drives this movement of the blood from its motionless state before it leaves the capillaries and begins its journey back to the heart? Is it possible that this force is the “pumping” of the heart? Wouldn’t there have to be some pump located in the capillaries propelling the blood forward and upward? Is there some “vital” force located in the capillaries that does this pumping? These are the questions we must grapple with if we’re going to understand how the blood circulates in the body. But one thing is clear: If the blood has stopped moving inside the capillaries, then the force cannot come from the heart. It must arise in the capillaries. (Thomas Cowan)
What’s amazing is that blood actually stops moving in the capillaries, which is necessary for the efficient exchange of gases, nutrients, and waste products. After the blood stops moving, it oscillates slightly, and then begins to flow again as it enters the veins. But if the blood stops moving at the midpoint of its circular flow through blood vessels, only then to start moving again, what is the force that drives this movement of the blood from its motionless state before it leaves the capillaries and begins its journey back to the heart? Is it possible that this force is the “pumping” of the heart? Wouldn’t there have to be some pump located in the capillaries propelling the blood forward and upward? Is there some “vital” force located in the capillaries that does this pumping? These are the questions we must grapple with if we’re going to understand how the blood circulates in the body. But one thing is clear: If the blood has stopped moving inside the capillaries, then the force cannot come from the heart. It must arise in the capillaries. (Thomas Cowan)
The Heart As Seen In The Iris
The heart area in the iris remains unchanged today. It is found in the exact position as given by the original discoverer of Iridology, Ignatz von Peczely. He produced the first chart of the iris which was published in a homoeopathic publication in Berlin, Germany, in 1884. The heart area appears in this chart in the exact position as found in the charts of today; it has been verified down through the years by such eminent iridologists as Liljequist, Thiel, Schlegel, Zoeppritz, Felke, Schnabel, Lane, Kritzer, Collins, Petinak, Maubach, and Jensen.
In the diagnosis of heart conditions we consider that Iridology is of extreme value; we can detect heart defects in their infancy – in the very first stages of inflammation. We can also detect if the condition is of an inherent nature. We can detect any destruction of tissue, as well as any distortion of same. The chronicity of severe conditions is revealed in the iris in an unmistakable manner.
Iris Areas – Reflexes, Affairs of the Heart by R.M. McLain, excerpted from Bernard Jensen's Iridology The Science and Practice in the Healing Arts, Volume 2
In the diagnosis of heart conditions we consider that Iridology is of extreme value; we can detect heart defects in their infancy – in the very first stages of inflammation. We can also detect if the condition is of an inherent nature. We can detect any destruction of tissue, as well as any distortion of same. The chronicity of severe conditions is revealed in the iris in an unmistakable manner.
Iris Areas – Reflexes, Affairs of the Heart by R.M. McLain, excerpted from Bernard Jensen's Iridology The Science and Practice in the Healing Arts, Volume 2
Locate the heart in the left iris, snuggled up against the autonomic nerve wreath, adjacent to the descending colon.
While a secondary location is also recognized in the right iris (as noted by German Iridologist Joseph Deck and commented by Farida Sharan in her book Iridology, a Complete Guide,) the bulk of research and case studies available are from Jensen, who recognized the heart's location exclusively in the left iris.
Presented here are three 'greats' perspectives on the heart: Bernard Jensen, Dorothy Hall, and Farida Sharan:
While a secondary location is also recognized in the right iris (as noted by German Iridologist Joseph Deck and commented by Farida Sharan in her book Iridology, a Complete Guide,) the bulk of research and case studies available are from Jensen, who recognized the heart's location exclusively in the left iris.
Presented here are three 'greats' perspectives on the heart: Bernard Jensen, Dorothy Hall, and Farida Sharan:
Iridology Explorers
Bernard Jensen
Some types of heart disturbances are associated with problems in the nerve supply. Other conditions are not related to the nerve supply at all. Two examples of the latter type are muscular problems and vascular obstructive problems. Usually, vascular obstructive problems are the ones associated with the common angina pain and heart attack we have become so familiar with. These are not heart problems as much as they are vascular problems that can have a chronic, or sometimes sudden, effect on an otherwise healthy heart.
Cardiovascular conditions do not generally reveal themselves in the heart area on the Iris chart. In addition, neither do they manifest as a disturbance of the autonomic nerve wreath, as do inherited weaknesses associated with nerve supply to the heart. Inherited heart weaknesses involving nerve supply manifest as a separation of the nerve wreath in the heart area. Please notice on the Iris chart that the heart and the solar plexus do not merely border the nerve wreath but are actually an integral part of it.
The iris sign to look for concerning an inherited heart weakness involving the nerve supply to this vital organ is a separation of the autonomic nerve wreath with a joining again in the heart area of the Iris chart. This produces a diamond shaped or trapezoidal shaped lesion where the wreath separation occurs. It is like a river sliding into two equal sized streams that unite again after forming a diamond shaped island in midstream. As with other lesions, you can check this island for an acute, chronic, or degenerative appearance. However, you must be extremely cautious not to mistake a dark bowel pocket opposite the heart area for a chronic or degenerative heart lesion. Even the experienced iridologist sometimes has trouble distinguishing between a bowel pocket and a heart lesion.
(Bernard Jensen)
Cardiovascular conditions do not generally reveal themselves in the heart area on the Iris chart. In addition, neither do they manifest as a disturbance of the autonomic nerve wreath, as do inherited weaknesses associated with nerve supply to the heart. Inherited heart weaknesses involving nerve supply manifest as a separation of the nerve wreath in the heart area. Please notice on the Iris chart that the heart and the solar plexus do not merely border the nerve wreath but are actually an integral part of it.
The iris sign to look for concerning an inherited heart weakness involving the nerve supply to this vital organ is a separation of the autonomic nerve wreath with a joining again in the heart area of the Iris chart. This produces a diamond shaped or trapezoidal shaped lesion where the wreath separation occurs. It is like a river sliding into two equal sized streams that unite again after forming a diamond shaped island in midstream. As with other lesions, you can check this island for an acute, chronic, or degenerative appearance. However, you must be extremely cautious not to mistake a dark bowel pocket opposite the heart area for a chronic or degenerative heart lesion. Even the experienced iridologist sometimes has trouble distinguishing between a bowel pocket and a heart lesion.
(Bernard Jensen)
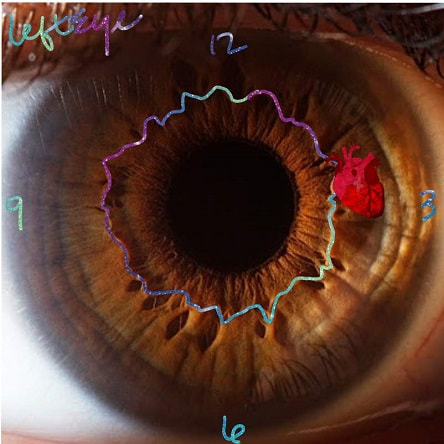
On the Iridology Chart the heart area is located in the left iris at three o'clock in zone 3, usually on the autonomic nerve wreath line. At times, it appears enclosed within the nerve wreath, and in other cases, it may be moved slightly to one side. The area of the aorta is directly above the heart within the autonomic wreath, which may seem to be split in case of aortic pathology. When we examine the heart area of the iris, we look for inherent weakness, nerve strength, toxic conditions, and reflex effects from other organs. If the autonomic nerve wreath is pierced by a radii solaris in the heart area, inherent weakness is noted and not necessarily disease. The radii solaris may refer to weak nerve activity here or toxins draining toward the heart. In all kinds of cardiac pathology, we find the autonomic wreath is involved, which is a definitive means of distinguishing a cardiac problem from bronchial trouble (the bronchi are also in zone three).
Heart conditions viewed in the iris will vary from one individual to another, and it is only by evaluating the condition of all organs and tissues in the irides that the iridologist can begin to understand the condition of the heart and the source or sources of the problem. This kind of understanding can only be gained through experience. The nerves, the lymph, the bowel, the psychological aspect and many other conditions affect the heart. (Bernard Jensen – Volume 2)
Heart conditions viewed in the iris will vary from one individual to another, and it is only by evaluating the condition of all organs and tissues in the irides that the iridologist can begin to understand the condition of the heart and the source or sources of the problem. This kind of understanding can only be gained through experience. The nerves, the lymph, the bowel, the psychological aspect and many other conditions affect the heart. (Bernard Jensen – Volume 2)
The most valuable resource on Iridology available: Bernard Jensen's Iridology The Science and Practice in the Healing Arts, Volume 2 (Unfortunately this original edition is out of print and has been altered in its reprinted form. Fortunately while rare and somewhat difficult to obtain (at times) there are still copies for sale in circulation.)
Dorothy Hall
For an iridologist to say 'heart’ rather than bronchial disturbance, many questions must be answered by the patient. Some severe viral attacks record massive disturbance over both zones, and the fuzzy iris, apparently out of focus no matter how you move the torch around, can often be recording a viral invasion which has flattened the patient altogether. Anesthetic shock can be felt severely by some people, and long after the operation a streak of grey or a fibre parting can still be seen. This can be so especially if an adrenaline injection has been given to pull the patient out of post- operative collapse. An electric shock can still remain obviously in the heart zone long afterwards, too.
I'm convinced the heart has a ‘memory’ system as well as the head. It stores the impression of trauma, and repeated shocks can stop it altogether as it refuses to meet the same negative stimuli. It is subjecting the heart to sudden loads rather than weakening it by too much stress and strain that does the damage. It is a rhythmical system in there, and disturbance of the harmony of counterpoint upsets it more than allegro speeds.
It is quite possible to die from a ‘broken heart’! Grief can be recorded here in a grey streak of misery and loss. So can the troubles of a dearly loved-one record in the heart zone. I have seen many patients showing classic heart disturbance signs in the iris, though all medical tests reveal no abnormality. Unclosed questioning, I find that a beloved husband, or wife, or child, or parent, has recently been a 'load’ which that patient has attempted to carry. A serious operation on the husband can produce a heart stress in his wife, and her iris records it as such.
A heart ‘attack’ can also be called by caused by an over-full bowel. The descending colon joins the heart area, and a sluggish elimination pattern can cause heart stress, even fatty degeneration of the heart as a muscle. See how important it can be to keep the bowels clean, and cleared often? Congestive heart failure can have one cause in chronic constipation. Folk who only have a bowel movement every four or five days may be told by a medical man: ‘Well, it's not causing you any obvious problems. Just don't worry about it.’ It's the non-obvious chronic enlargement of the colon that can one day pressure your heart into feeling it is sick!
‘Heart-sick’ people are more common than cardiac patients. Many of those in hospital wards are there after emotionally triggered burdens become too heavy period the iris can tell a professionally trained person the story. (Dorothy Hall)
I'm convinced the heart has a ‘memory’ system as well as the head. It stores the impression of trauma, and repeated shocks can stop it altogether as it refuses to meet the same negative stimuli. It is subjecting the heart to sudden loads rather than weakening it by too much stress and strain that does the damage. It is a rhythmical system in there, and disturbance of the harmony of counterpoint upsets it more than allegro speeds.
It is quite possible to die from a ‘broken heart’! Grief can be recorded here in a grey streak of misery and loss. So can the troubles of a dearly loved-one record in the heart zone. I have seen many patients showing classic heart disturbance signs in the iris, though all medical tests reveal no abnormality. Unclosed questioning, I find that a beloved husband, or wife, or child, or parent, has recently been a 'load’ which that patient has attempted to carry. A serious operation on the husband can produce a heart stress in his wife, and her iris records it as such.
A heart ‘attack’ can also be called by caused by an over-full bowel. The descending colon joins the heart area, and a sluggish elimination pattern can cause heart stress, even fatty degeneration of the heart as a muscle. See how important it can be to keep the bowels clean, and cleared often? Congestive heart failure can have one cause in chronic constipation. Folk who only have a bowel movement every four or five days may be told by a medical man: ‘Well, it's not causing you any obvious problems. Just don't worry about it.’ It's the non-obvious chronic enlargement of the colon that can one day pressure your heart into feeling it is sick!
‘Heart-sick’ people are more common than cardiac patients. Many of those in hospital wards are there after emotionally triggered burdens become too heavy period the iris can tell a professionally trained person the story. (Dorothy Hall)
Farida Sharan
Heart The circulatory system in the iris - Although western iris charts show the heart area only in the left eye, it also appears in the right iris from 9:30-10:00 o’clock. Whenever strong heart signs appear, also check out the right heart signs. Josef Deck in the recent translation of his Principles of Iris Diagnosis differentiates the left heart and the right heart and maintains that ‘insufficiency of the heart' is indicated by a constitutional marking at 2:30 and at 3:30 on the left. Marking in the zone of 2:00 o’clock on the iris collarette indicates aortic insufficiency. Small markings in the heart zone indicate defects, resolved quiescent infarcts or toxic damage. Markings between 3 and 4 o’clock in the pulmonary sector are sometimes very prominent especially in pulmonary congestion with cardiac insufficiency.’ (Farida Sharan)
The Golden Heart
The golden ratio, or golden mean, of 1.618 is a proportion known since antiquity to be the most aesthetically pleasing and has been used repeatedly in art and architecture. Both the golden ratio and the allied golden angle of 137.5° have been found within the proportions and angles of the human body and plants. In the human heart we found many applications of the golden ratio and angle, in addition to those previously described. In healthy hearts, vertical and transverse dimensions accord with the golden ratio, irrespective of different absolute dimensions due to ethnicity. In mild heart failure, the ratio of 1.618 was maintained but in end-stage heart failure the ratio significantly reduced. Similarly, in healthy ventricles mitral annulus dimensions accorded with the golden ratio, while in dilated cardiomyopathy and mitral regurgitation patients the ratio had significantly reduced. In healthy patients, both the angles between the mid-luminal axes of the pulmonary trunk and the ascending aorta continuation and between the outflow tract axis and continuation of the inflow tract axis of the right ventricle approximate to the golden angle, although in severe pulmonary hypertension, the angle is significantly increased. Hence the overall cardiac and ventricular dimensions in a normal heart are consistent with the golden ratio and angle, representing optimum pump structure and function efficiency, whereas there is significant deviation in the disease state. These findings could have anatomical, functional and prognostic value as markers of early deviation from normality. (6)
Botanical Healers
Cardiotonic or Cardioactive? In a strictly technical sense, the pharmacological term cardiotonic is synonymous with "positive inotropic." In pharmacology, the word cardiotonic is used not only to describe agents that increase contractility, but also to indicate an increase in frequency, an increase in the beat volume, or a general increase in cardiac performance. In the phytotherapeutic literature, however, slightly different terminology is used. Here, cardioactive plants are those that owe their effects on the heart to cardiac glycosides or other very active substances; they thus possess both the strengths and the drawbacks of these constituents. An example is Digitalis (foxglove). Cardiotonic plants, on the other hand, are those that have an observable beneficial action on the heart and blood vessels but contain no cardiac glycosides, such as Crataegus (hawthorn). The mechanisms behind their actions are obscure and constitute a subject of considerable pharmacological debate.
The medical herbalist recognizes a broad range of relevant herbs for the cardiovascular system. As a group, they are known as cardiac remedies, a general term for herbs that have an action on the heart. Some of the remedies in this group are powerful cardioactive agents, such as Digitalis spp. (foxglove) and the somewhat milder Comvallaria majalis (lily of the valley), while others are gentler and safer cardiotonics, such as Crataegus (hawthorn) and Tilia (linden flower).
Cardioactive herbs owe their effects on the heart to highly active substances, such as cardiac glycosides, and thus have both the strengths and drawbacks of these powerful constituents. Cardiotonics have a beneficial action on the heart and blood vessels, but do not contain cardiac glycosides. While they do not offer the dramatic, rapid, and often life-saving benefits of many of the drugs used in modern cardiology, cardiotonics confer a definite advantage in the treatment or prevention of chronic degenerative conditions. (David Hoffman, Medical Herbalism)
Cardioactive herbs owe their effects on the heart to highly active substances, such as cardiac glycosides, and thus have both the strengths and drawbacks of these powerful constituents. Cardiotonics have a beneficial action on the heart and blood vessels, but do not contain cardiac glycosides. While they do not offer the dramatic, rapid, and often life-saving benefits of many of the drugs used in modern cardiology, cardiotonics confer a definite advantage in the treatment or prevention of chronic degenerative conditions. (David Hoffman, Medical Herbalism)
Herbs considered important for the cardiovascular system are classified according to traditional actions of cardioactive, cardioprotective, cardiotonic, and circulatory stimulants. Anticoagulants are a more modern application of herbs to cardiovascular disease and nervines and diuretic herbs are traditionally included in formulas. (8) http://medicinalplants.us/
Cardioactive herbs
Cardioactive herbs are some of the most potentially toxic herbs. Many of these contain cardioactive glycosides such as Foxglove (Digitalis purpurea) and Lily of the Valley (Convallaria majalis), which are ionotropic and lead to a more efficient and coordinated cardiac contraction. Perhaps the most useful is Bugleweed (Lycopus europaeus, L. virginicus). It does not contain cardiac glycosides but is still cardioactive. L. virginicus was recognized by the early Eclectics as an excellent sedative with properties similar to digitalis but without adverse side effects.
Cardioprotective herbs
Cardioprotective herbs are used by herbalists to reduce the risk of damage due to ischemia or toxins. Potential actions include increasing cardiac blood flow, raising intracellular levels of cAMP, reducing capillary fragility, reducing peripheral vascular resistance through vasorelaxant activity, reducing cholesterol, and reducing hypertension. These herbs are generally rich in flavonoids, providing antioxidant benefits for systems undergoing oxidative stress. Perhaps the best known and used cardioprotective herb is Hawthorn (Crataegus spp), although it is also mildly cardiotonic and possibly even mildly cardioactive. Its activity has been attributed to the flavonoid components, particularly the procyanidins.
Cardioactive herbs are some of the most potentially toxic herbs. Many of these contain cardioactive glycosides such as Foxglove (Digitalis purpurea) and Lily of the Valley (Convallaria majalis), which are ionotropic and lead to a more efficient and coordinated cardiac contraction. Perhaps the most useful is Bugleweed (Lycopus europaeus, L. virginicus). It does not contain cardiac glycosides but is still cardioactive. L. virginicus was recognized by the early Eclectics as an excellent sedative with properties similar to digitalis but without adverse side effects.
Cardioprotective herbs
Cardioprotective herbs are used by herbalists to reduce the risk of damage due to ischemia or toxins. Potential actions include increasing cardiac blood flow, raising intracellular levels of cAMP, reducing capillary fragility, reducing peripheral vascular resistance through vasorelaxant activity, reducing cholesterol, and reducing hypertension. These herbs are generally rich in flavonoids, providing antioxidant benefits for systems undergoing oxidative stress. Perhaps the best known and used cardioprotective herb is Hawthorn (Crataegus spp), although it is also mildly cardiotonic and possibly even mildly cardioactive. Its activity has been attributed to the flavonoid components, particularly the procyanidins.
Fruits & Foods
Leafy green vegetables
Leafy green vegetables like spinach, kale, and collard greens are well known for their wealth of vitamins, minerals, and antioxidants.
In particular, they’re a great source of vitamin K, which helps protect your arteries and promote proper blood clotting.
They’re also high in dietary nitrates, which have been shown to reduce blood pressure, decrease arterial stiffness, and improve the function of cells lining the blood vessels. (9)
Some studies have also found a link between increasing your intake of leafy green vegetables and a lower risk of heart disease.
One analysis of eight studies found that increasing leafy green vegetable intake was associated with up to a 16% lower incidence of heart disease. (10)
Another study in 29,689 women showed that a high intake of leafy green vegetables was linked to a significantly lower risk of coronary heart disease. (11)
Berries
Strawberries, blueberries, blackberries, and raspberries are jam-packed with important nutrients that play a central role in heart health.
Berries are also rich in antioxidants like anthocyanins, which protect against the oxidative stress and inflammation that contribute to the development of heart disease.
Studies show that eating lots of berries can reduce several risk factors for heart disease.
For example, one study in 33 adults with obesity showed that consuming strawberries at two and a half servings for 4 weeks significantly improved insulin resistance and LDL (bad) cholesterol. (12)
Another study found that eating blueberries daily improved the function of cells that line the blood vessels, which help control blood pressure and blood clotting (11Trusted Source).
Additionally, an analysis of 22 studies showed that eating berries was associated with reductions in LDL (bad) cholesterol, systolic blood pressure, body mass index, and certain markers of inflammation (12Trusted Source).
Berries can be a satisfying snack or delicious low calorie dessert. Try adding a few different types to your diet to take advantage of their unique health benefits.
Avocados
Avocados are an excellent source of heart-healthy monounsaturated fats, which have been linked to reduced levels of cholesterol and a lower risk of heart disease.
One study looked at the effects of three cholesterol-lowering diets in 45 people with overweight and obesity, with one of the test groups consuming one avocado per day.
The avocado group experienced reductions in LDL (bad) cholesterol, including lower levels of small, dense LDL (bad) cholesterol, which is believed to significantly raise the risk of heart disease.
The lipid-lowering and cardioprotective effects of avocado have been demonstrated in several studies.
Avocados are also rich in potassium, a nutrient that’s essential to heart health. In fact, just one avocado supplies 975 milligrams of potassium, or about 28% of the amount that you need in a day.
Getting at least 4.7 grams of potassium per day can decrease blood pressure by an average of 8.0/4.1 mmHg, which is associated with a 15% lower risk of stroke.
Tomatoes
Tomatoes are loaded with lycopene, a natural plant pigment with powerful antioxidant properties.
Antioxidants help neutralize harmful free radicals, preventing oxidative damage and inflammation, both of which can contribute to heart disease.
Low blood levels of lycopene are linked to an increased risk of heart attack and stroke.
Increasing the intake of tomato products and lycopene supplementation have positive effects on blood lipids, blood pressure, and endothelial function.
Another study in 50 women with overweight found that eating two raw tomatoes four times per week increased levels of HDL (good) cholesterol.
Higher levels of HDL (good) cholesterol can help remove excess cholesterol and plaque from the arteries to keep your heart healthy and protect against heart disease and stroke.
Leafy green vegetables like spinach, kale, and collard greens are well known for their wealth of vitamins, minerals, and antioxidants.
In particular, they’re a great source of vitamin K, which helps protect your arteries and promote proper blood clotting.
They’re also high in dietary nitrates, which have been shown to reduce blood pressure, decrease arterial stiffness, and improve the function of cells lining the blood vessels. (9)
Some studies have also found a link between increasing your intake of leafy green vegetables and a lower risk of heart disease.
One analysis of eight studies found that increasing leafy green vegetable intake was associated with up to a 16% lower incidence of heart disease. (10)
Another study in 29,689 women showed that a high intake of leafy green vegetables was linked to a significantly lower risk of coronary heart disease. (11)
Berries
Strawberries, blueberries, blackberries, and raspberries are jam-packed with important nutrients that play a central role in heart health.
Berries are also rich in antioxidants like anthocyanins, which protect against the oxidative stress and inflammation that contribute to the development of heart disease.
Studies show that eating lots of berries can reduce several risk factors for heart disease.
For example, one study in 33 adults with obesity showed that consuming strawberries at two and a half servings for 4 weeks significantly improved insulin resistance and LDL (bad) cholesterol. (12)
Another study found that eating blueberries daily improved the function of cells that line the blood vessels, which help control blood pressure and blood clotting (11Trusted Source).
Additionally, an analysis of 22 studies showed that eating berries was associated with reductions in LDL (bad) cholesterol, systolic blood pressure, body mass index, and certain markers of inflammation (12Trusted Source).
Berries can be a satisfying snack or delicious low calorie dessert. Try adding a few different types to your diet to take advantage of their unique health benefits.
Avocados
Avocados are an excellent source of heart-healthy monounsaturated fats, which have been linked to reduced levels of cholesterol and a lower risk of heart disease.
One study looked at the effects of three cholesterol-lowering diets in 45 people with overweight and obesity, with one of the test groups consuming one avocado per day.
The avocado group experienced reductions in LDL (bad) cholesterol, including lower levels of small, dense LDL (bad) cholesterol, which is believed to significantly raise the risk of heart disease.
The lipid-lowering and cardioprotective effects of avocado have been demonstrated in several studies.
Avocados are also rich in potassium, a nutrient that’s essential to heart health. In fact, just one avocado supplies 975 milligrams of potassium, or about 28% of the amount that you need in a day.
Getting at least 4.7 grams of potassium per day can decrease blood pressure by an average of 8.0/4.1 mmHg, which is associated with a 15% lower risk of stroke.
Tomatoes
Tomatoes are loaded with lycopene, a natural plant pigment with powerful antioxidant properties.
Antioxidants help neutralize harmful free radicals, preventing oxidative damage and inflammation, both of which can contribute to heart disease.
Low blood levels of lycopene are linked to an increased risk of heart attack and stroke.
Increasing the intake of tomato products and lycopene supplementation have positive effects on blood lipids, blood pressure, and endothelial function.
Another study in 50 women with overweight found that eating two raw tomatoes four times per week increased levels of HDL (good) cholesterol.
Higher levels of HDL (good) cholesterol can help remove excess cholesterol and plaque from the arteries to keep your heart healthy and protect against heart disease and stroke.
Watermelon
Exciting new areas of study suggest that an amino acid called L-citrulline (286- 1266 mg per 2 cup serving) in watermelon may help to support vascular health and help maintain healthy blood flow. Larger and longer term studies are needed to demonstrate this effect in other populations.
Another exciting area of study is the role of lycopene (a carotenoid found in watermelon and other red produce) in maintaining heart health. Lycopene (12.7 grams of lycopene per 2 cup serving) has been studied for its potential to reduce blood pressure in those with prehypertension or hypertension. www.watermelon.org/nutrition/watermelons-benefits/
Exciting new areas of study suggest that an amino acid called L-citrulline (286- 1266 mg per 2 cup serving) in watermelon may help to support vascular health and help maintain healthy blood flow. Larger and longer term studies are needed to demonstrate this effect in other populations.
Another exciting area of study is the role of lycopene (a carotenoid found in watermelon and other red produce) in maintaining heart health. Lycopene (12.7 grams of lycopene per 2 cup serving) has been studied for its potential to reduce blood pressure in those with prehypertension or hypertension. www.watermelon.org/nutrition/watermelons-benefits/
"On every level, including biochemically, melon is exactly what our bodies need. Melons are essentially balls of purified water. This highly active fluid binds onto poisons of all kinds in the body, including mold, mycotoxins, viral neurotoxins, undigested protein toxins, ammonia gas, and bacterial toxins, flushing them out to allow the immune system to restore itself. Further, the fruit’s high electrolyte content helps protect the brain and the rest of the nervous system from stress-related strokes, aneurysms, and embolisms. Melon thins the blood and reduces heart attack risk, helps prevent heart disease and vascular issues, and can even reduce liver and kidney disease—if someone is suffering from liver or kidney malfunction, melon can mean the difference between life and death. The water in melon is nearly identical to our blood, and its sodium, potassium, and glucose are also abundant and bioavailable, making melon one of the most hydrating foods you can eat. This hydration is critical, as it helps to lower high blood pressure, among other benefits." (Medical Medium)
Resources & Recommended
Additional Resources:
1. https://www.cosmic-core.org/free/article-197-human-ap-part-4-the-geometry-of-human-life-the-heart/
2. "The Heart is Not a Pump: A Refutation of the Pressure Control Premise of Heart Function" by Ralph Marinelli (pdf version available)
3. http://frankchester.com/the-heart/
4. Juan Cosín Aguilar Centro de Investigación La Fe, Valencia, Spain. https://icvd-kcs.org/sources/torrent_guasp.pdf)
5. https://www.pbs.org/wgbh/americanexperience/features/partners-heart-history/
6. https://pubmed.ncbi.nlm.nih.gov/21703707
7. https://www.healthline.com/nutrition/heart-healthy-foods
(8) http://medicinalplants.us/
(9) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4288952/
(10) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4973479/
(11) https://pubmed.ncbi.nlm.nih.gov/21177799/
(12) https://pubmed.ncbi.nlm.nih.gov/33922576/
2. "The Heart is Not a Pump: A Refutation of the Pressure Control Premise of Heart Function" by Ralph Marinelli (pdf version available)
3. http://frankchester.com/the-heart/
4. Juan Cosín Aguilar Centro de Investigación La Fe, Valencia, Spain. https://icvd-kcs.org/sources/torrent_guasp.pdf)
5. https://www.pbs.org/wgbh/americanexperience/features/partners-heart-history/
6. https://pubmed.ncbi.nlm.nih.gov/21703707
7. https://www.healthline.com/nutrition/heart-healthy-foods
(8) http://medicinalplants.us/
(9) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4288952/
(10) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4973479/
(11) https://pubmed.ncbi.nlm.nih.gov/21177799/
(12) https://pubmed.ncbi.nlm.nih.gov/33922576/